Getting told your LDL is too high can be unsettling, especially when the conversation quickly turns toward heart disease risk and medication. Most people are left with the impression that one number on a standard lipid panel has already told them everything important. But that is not really how cardiovascular risk works. A basic cholesterol test can raise useful questions, but by itself it cannot tell you the full story about what is happening in your arteries.
That does not mean your doctor is automatically wrong, and it does not mean LDL is meaningless. It means the picture is often more nuanced than people are led to believe. LDL-C is only one marker. It does not directly show plaque, it does not tell you how many atherogenic particles are actually present, and it does not reveal the wider metabolic and inflammatory environment those particles are moving through.
That is why newer guidance has moved beyond LDL-C alone, adding tests like apoB to better reflect particle burden, Lp(a) to uncover inherited risk, and coronary artery calcium scoring (CAC) when a more direct look at plaque may help clarify the situation.
This article is here to help you make sense of that bigger picture. Not to tell you to ignore your doctor, and not to tell you what decision to make, but to help you understand what HDL, LDL, and triglyceride measures can and cannot actually tell you before you make one.
By the end, you should have a clearer sense of what LDL, HDL, and triglycerides really measure, why LDL alone is not a full risk picture, and which other markers can give a more useful read on atherosclerosis risk.
Why Cholesterol Numbers Can Be Confusing
Cholesterol numbers can be confusing because most people are given a very simple message about a much more complicated picture.
Usually, the story goes something like this: LDL is the “bad” cholesterol, HDL is the “good” cholesterol, and triglycerides are another number you want to keep low. That sounds clear enough, until someone gets their blood test back and realizes the numbers do not always fit neatly into that story.
One person may have high LDL but low triglycerides and decent HDL. Another may have “normal” LDL but high triglycerides and low HDL. Someone else may be told their cholesterol looks fine, even though other problems may be developing beneath the surface. At that point, the usual good-versus-bad labels stop being very helpful.
Part of the confusion is that the doctor’s favorite standard lipid panel test can only tell you so much. It may point to patterns worth paying attention to, but it cannot show whether the artery wall is inflamed, whether LDL is being oxidized, or whether plaque is actively developing. It can suggest risk, but it cannot reveal the condition of the arteries themselves.
What a Standard Lipid Panel Measures
| Marker | What it measures | Why people focus on it | What it does not tell you by itself |
| Total Cholesterol | Your overall cholesterol level | Gives a broad overview | Whether that cholesterol is in a favorable or unfavorable pattern |
| LDL-C | The amount of cholesterol being carried inside LDL particles | Often used as the main “risk” number | How many LDL particles you have, whether they are being oxidized, or whether plaque is present |
| HDL-C | The amount of cholesterol being carried in HDL particles | Often called “good” cholesterol because HDL helps carry cholesterol back to the liver | Whether you are truly protected from heart disease |
| Triglycerides | The amount of fat circulating in your blood | Can reflect metabolic health, insulin resistance, and energy overload | Whether plaque is present in the arteries |
As a result, cholesterol numbers can be (and often are) read too simplistically. A high LDL result on its own may cause alarm, even when the wider metabolic picture looks healthy. On the other hand, a person with lower LDL may be given reassurance, even though inflammation, oxidation, or metabolic dysfunction are still present. The numbers are not useless, but they are not the whole story either.
This is where many people get stuck. They are told one number is too high or one number looks fine, but they are not told what those results can and cannot actually reveal. That is why cholesterol discussions often create more confusion than clarity. To make sense of these markers, you need more than a label. You need context.
What LDL, HDL, and Triglycerides Actually Measure
One reason cholesterol results can be so confusing is that a standard lipid panel does not directly show whether your arteries are healthy or diseased. It does not show plaque, and it does not tell you the full number of atherogenic particles moving through your bloodstream. What it mainly tells you is how much cholesterol and fat is being carried in the blood.
That still matters, but these markers are not all measuring the same thing. LDL and HDL are lipoproteins that carry cholesterol, while triglycerides are a form of fat the body uses and stores for energy. So although these numbers often get grouped together on one blood test, they each tell you something slightly different. Understanding that is the first step to making sense of what your results actually mean.
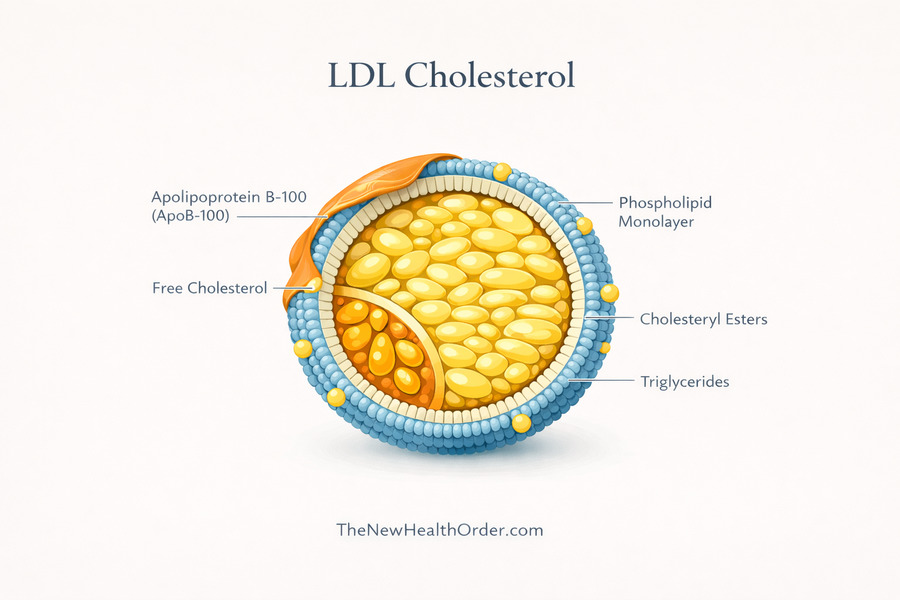
LDL Cholesterol
LDL is short for low-density lipoprotein. Its main job is to carry cholesterol through the bloodstream and deliver it to tissues that need it. Cholesterol itself is not the enemy—our body needs it for cell membranes, hormones, vitamin D, and other essential functions.
The reason LDL gets so much attention is that higher LDL levels usually mean greater exposure to particles that can contribute to plaque formation over time (called atherogenic particles). But LDL does not act in isolation. Whether those particles become part of the problem depends on the wider context, including particle burden, metabolic health, inflammation, and what is happening inside the artery wall itself before cholesterol even gets there.
That is why LDL is often called “bad” cholesterol, but that label is too simple. LDL is not bad because cholesterol delivery is bad. It gets that label because LDL-related particles are involved in atherosclerosis under the wrong conditions and over time. A low LDL result does not automatically mean everything is fine, and a higher LDL result does not tell the whole story by itself. LDL is better understood as one important marker within a bigger cardiovascular picture.
For a deeper look into cholesterol and whether it really is “bad” for you, see this article here.
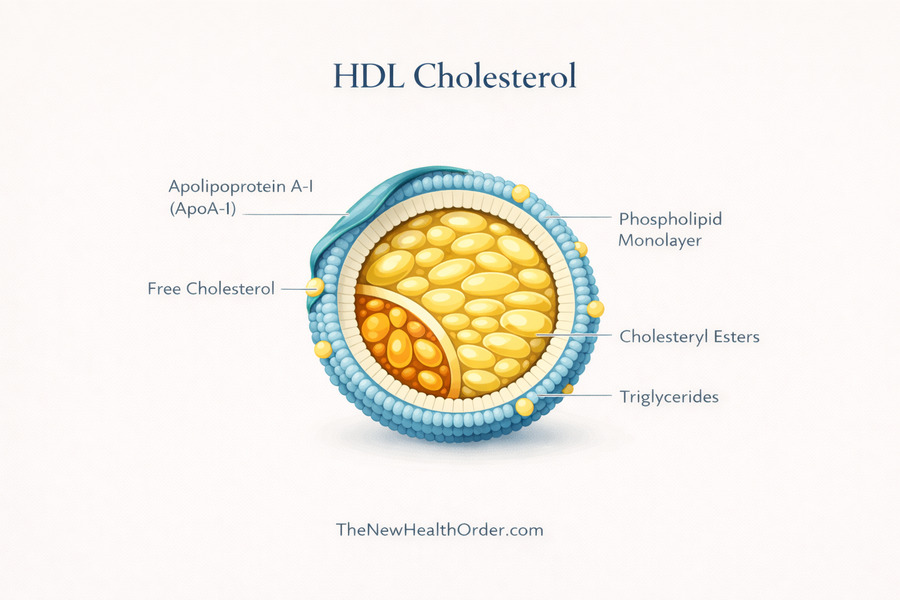
HDL Cholesterol
HDL stands for high-density lipoprotein. It is often described as the “good” cholesterol because it helps carry cholesterol away from tissues and back to the liver, where it can be reused or removed from the body. That reverse transport role is why higher HDL has traditionally been seen as protective.
But HDL is not as simple as “higher is always better.” A healthy HDL level may be a helpful sign but it does not cancel out every other concern on a blood test. A person can have a decent HDL and still have other problems developing out of sight. So while HDL can point in a favorable direction, it is better thought of as one more piece of context rather than an automatic shield against heart disease.
Triglycerides
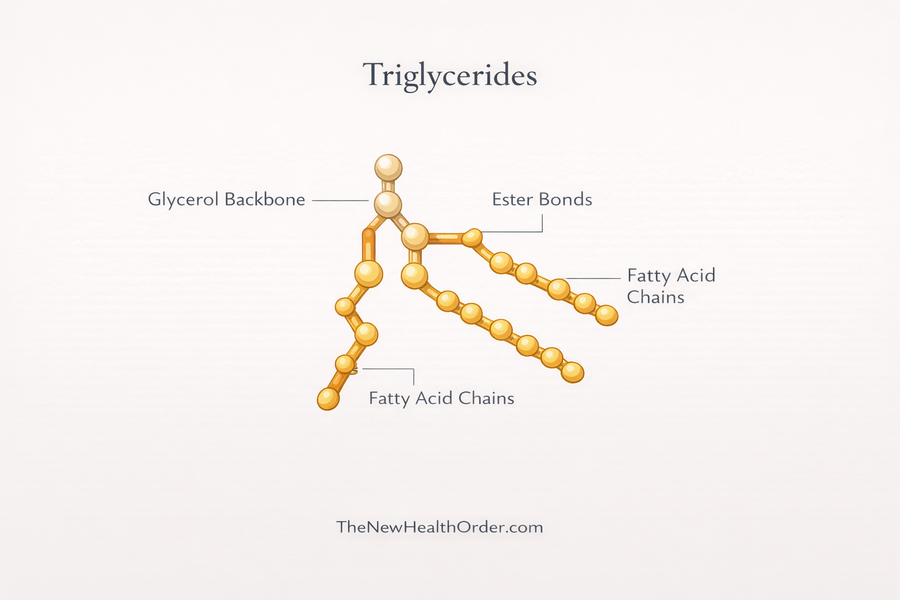
Triglycerides are different from LDL and HDL since they are not mainly about transporting cholesterol. They are the most common type of fat in the body, and one of their main roles is energy storage. When you consume more energy than your body needs right away, much of that excess can be converted into triglycerides and stored in fat cells for later use.
That is why triglycerides can tell you something important about metabolic health. Elevated triglycerides often suggest that the body is not handling energy especially well, particularly when they show up alongside low HDL. MedlinePlus notes that triglycerides of 150 mg/dL or higher are a risk factor for metabolic syndrome, and the American Heart Association notes that high triglycerides combined with high LDL or low HDL are linked with fatty buildup in artery walls.
This is what makes triglycerides a useful clue. LDL is usually the number people focus on, but triglycerides can sometimes say more about the underlying metabolic picture. If they are high, especially in the context of low HDL, that may point toward insulin resistance, excess energy intake, or broader metabolic dysfunction rather than just a cholesterol transport issue.
Taken together, these three markers help sketch out part of the picture. LDL tells you about cholesterol being delivered in the blood. HDL gives some sense of cholesterol being carried back toward the liver. Triglycerides tell you more about stored energy and metabolic strain.
Useful? Yes. But complete? No. And that is exactly why interpreting a lipid panel is often more complicated than simply asking whether one number is high or low. And when a lifetime prescription of pharmaceutical interventions is on the line, you want to make sure you are actually treating something tangible.
Get Your Free Book!
Enter your email to get the free book and occasional updates from The New Health Order.
Why LDL Is Not the Whole Story
LDL gets a huge amount of attention in cholesterol discussions, and for understandable reasons. But one number on a blood test cannot tell you everything that matters about cardiovascular risk. To understand what a high LDL result may or may not mean, you have to look beyond the number itself and ask what is happening in the wider metabolic and arterial environment.
Why High LDL Is Not a Full Risk Picture
LDL-C is not a meaningless number. It can reflect part of the picture, and in some cases it may point toward greater exposure to lipoproteins that could become involved in plaque formation over time. But that does not mean LDL-C gives a complete or consistent picture on its own.
Population studies have not always shown a simple straight-line story, and some cohort data have found U-shaped or bell-shaped relationships between LDL-related measures and all-cause mortality, with worse outcomes at both the low and high ends. That does not prove high LDL is harmless, but does suggest the real situation is more complex than “higher is always worse” and “lower is always better.”
Part of the reason is that LDL-C is only measuring the amount of cholesterol being carried inside LDL particles. It does not tell you how many atherogenic particles are actually present, whether plaque is already forming, or what kind of environment those particles are moving through.
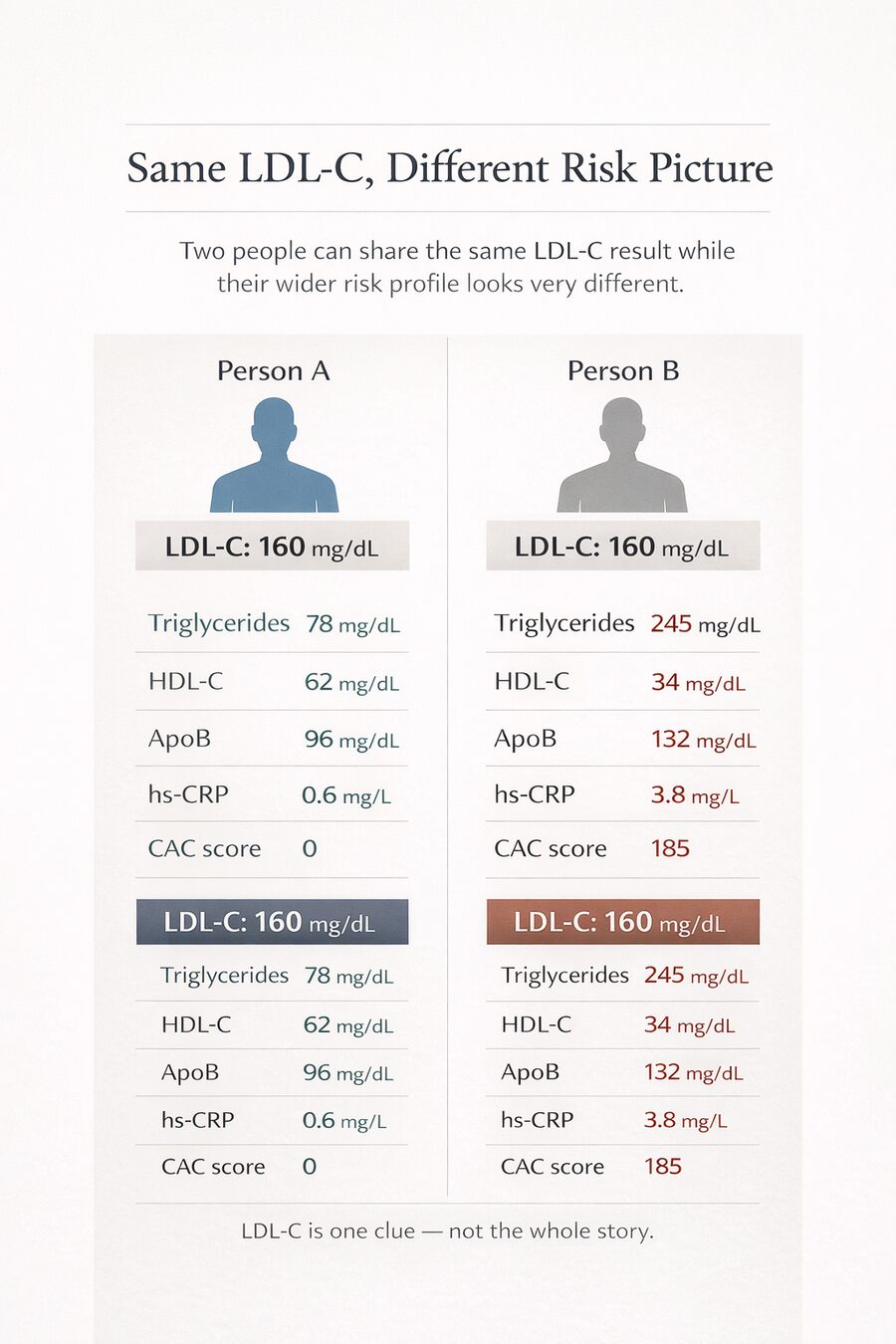
Recent discordance data show that people with the same LDL-C can have meaningfully different apoB levels and different event rates, which means the same LDL-C number can mean different things in different people.
That is why two people can have the same LDL-C result and still have very different cardiovascular pictures. One person may have low triglycerides, decent HDL, good metabolic health, and no obvious sign of wider dysfunction. Another may have the same LDL-C alongside insulin resistance, inflammation, elevated triglycerides, or other atherogenic factors. On paper, the LDL-C looks the same. In reality, the wider picture is not.
So the real takeaway is not that LDL-C is meaningless. It is that LDL-C is incomplete. It may point in an important direction, but by itself it cannot tell you exactly what is happening in the arteries, how inflamed the environment is, or how much risk a person truly carries. That is why a high LDL result deserves context and additional testing.
Why Oxidation and Inflammation Matter
LDL does not usually become a problem simply because it is present in the blood. The bigger issue is what kind of environment it is moving through. A healthy artery lining helps keep the vessel calm, smooth, and resistant to injury. But when that lining is irritated or dysfunctional — from things like high blood pressure, smoking, high blood sugar, insulin resistance, or ongoing oxidative stress — it becomes easier for LDL particles to move beneath the surface of the artery wall.
That is where retention comes in. LDL is not usually dangerous while it is simply passing by in the bloodstream. The problem begins when apoB-containing particles get trapped in the artery wall instead of moving on. Research on the response-to-retention model shows that these particles can bind to components of the artery wall called proteoglycans, which helps hold them in place. In simple terms, the artery wall becomes a place where LDL can linger rather than just circulate.
Once LDL is stuck there, it has more time to be changed by the local environment. Retained LDL is more prone to oxidation and other damaging modifications than LDL that keeps moving through the blood—important because modified LDL is much more likely to trigger immune activity, attract inflammatory cells, and help drive the plaque-building process.
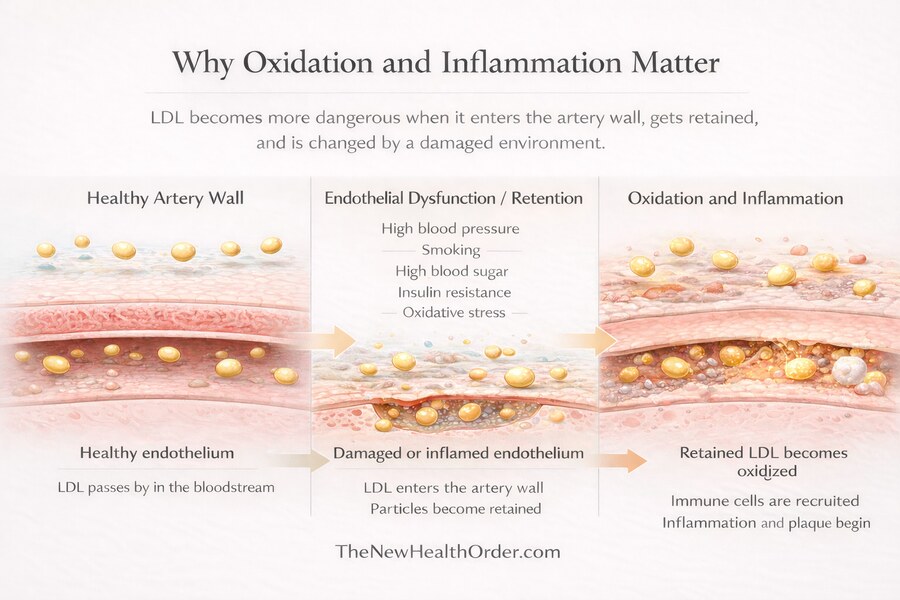
This is why the state of the artery wall matters so much. LDL is part of the story, but it is not the whole story. The deeper issue is that an unhealthy, inflamed, or damaged arterial environment makes retention more likely, and retention makes harmful modification more likely. That helps explain why LDL can look like the main villain, when in many cases it is being pulled into a process that started further upstream.
What Matters More Than One LDL Number
If someone really wants a clearer sense of their atherosclerosis risk, the better question is not just, “What is my LDL?” It is, “What else is going on around it?” That is where the wider pattern starts to matter — things like triglycerides, HDL, apoB, Lp(a), inflammation, and sometimes imaging that looks more directly for plaque.
Why High Triglycerides and Low HDL Matter
Triglycerides and HDL can tell you a lot about the environment LDL is showing up in. High triglycerides and low HDL often go hand in hand with insulin resistance and poorer metabolic health.
In simple terms, they can suggest that the body is not handling fuel especially well, which is important because atherosclerosis is not just about how much cholesterol is moving through the blood. It is also about the kind of metabolic setting that cholesterol is moving through. Triglycerides often act as a clue to insulin resistance and remnant-particle burden, while low HDL can be part of the same disturbed pattern.
This is why the same LDL number can mean different things in different people. High LDL alongside high triglycerides and low HDL is a more concerning pattern than high LDL with low triglycerides and decent HDL. It does not make LDL irrelevant in the second case. It just means the pattern around LDL gives that result more meaning.
Why ApoB May Be Better
An often overlooked detail about LDL-C values is that it tells you how much cholesterol is being carried inside LDL particles, not the number of particles themselves. ApoB is the metric that tells you how many atherogenic particles are actually there.
That difference matters more than it first sounds because people can have the same LDL-C, but one can be carrying many more particles than the other. And from an artery’s point of view, particle number may matter more than the total amount of cholesterol those particles happen to be carrying.
That is why apoB is one of the most useful follow-up tests when the standard panel feels incomplete. The 2026 guideline says apoB may be used to assess residual ASCVD risk and guide treatment in people with diabetes, high triglycerides, cardiovascular-kidney-metabolic syndrome, or known cardiovascular disease, and notes that it may be more accurate than LDL-C in those groups. Essentially, apoB gets closer to true particle burden and can reveal residual risk even when LDL-C does not look especially alarming.
Lp(a) – Lipoprotein-A
Lp(a) is useful because it helps uncover inherited risk that an ordinary lipid panel can miss. It is basically an LDL-like particle with an extra protein attached, and it is largely determined by genetics. Unfortunately, that means it is not the sort of number you usually fix with lifestyle alone, and it does not tend to fluctuate much over time.
This makes it especially helpful in people whose risk does not seem to match their standard cholesterol numbers, or in families where heart disease shows up early for reasons that are not obvious on a routine panel. Current guidance recommends measuring Lp(a) at least once in adulthood, and your research summary notes the same point while highlighting that high levels are considered a meaningful risk enhancer.
Coronary Artery Calcium Scan (CAC)
Some tests do not just estimate risk from the outside but build you a picture closer to the disease itself. A coronary artery calcium scan (CAC) is the clearest example. It looks for calcified plaque in the coronary arteries, which means it is no longer just asking whether the numbers suggest risk — it is asking whether there is evidence of plaque already being there. A CAC score of zero is associated with very low near-term risk, while higher scores point toward more plaque burden and a more concerning picture.
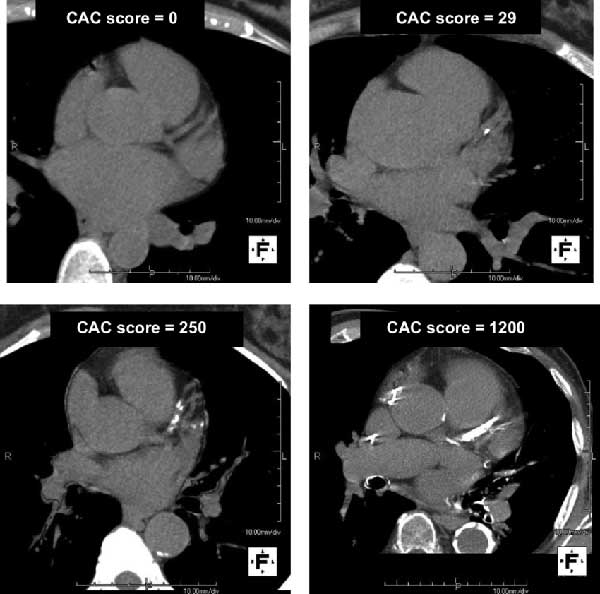
If I could do only one test to get the most useful single piece of information about the current coronary atherosclerosis burden, then CAC is probably the best single practical test, because it looks for actual calcified coronary plaque, not just risk factors in the blood, and higher CAC scores track strongly with future event risk.
Unfortunately, due to cost and logistics, current guidance uses CAC selectively, mainly for asymptomatic adults where the true risk is still uncertain after the usual clinical assessment, especially men 40+ and women 45+ with borderline or intermediate estimated risk.
While CAC is probably the best single validated test for estimating subclinical coronary plaque burden in many asymptomatic middle-aged adults, it is not the best single test for every person and it does not rule out all atherosclerosis, which is why you want to combine it with other tests.
Other Markers
Inflammation markers can add context too, but they need to be interpreted carefully. Hs-CRP is the most practical one. If it is high, it may suggest a more inflammatory background in the body, but it is not specific to the arteries and can be elevated for many unrelated reasons.
Just as importantly, a low hs-CRP does not prove the arteries are clean. It can lower suspicion a little, but it cannot rule out plaque on its own, which is why authorities like the ACC discuss hs-CRP as a useful risk-enhancer and modifier rather than a definitive test.
There is also a lot of talk around oxidized LDL. Mechanistically, it makes a lot of sense and fits the biology of how LDL can become more harmful once it is retained and modified in the artery wall. But as a real-world clinical test, it is still not especially useful for most people.
The problem is not that oxidized LDL is unimportant, it’s that the biology is easier to understand than it is to measure. What matters most is what is happening locally inside the artery wall, but a blood test can only measure what oxLDL is circulating in the bloodstream.
On top of that, oxidized LDL is not one single uniform substance, the tests are not fully standardized, and the results have not consistently outperformed more practical tools like apoB, Lp(a), or coronary calcium scoring. So oxidized LDL is highly important to the mechanism, but not yet one of the most useful routine tests in everyday practice.
| Marker | What It Measures | Predicts Best | Strengths | Limitations | When to Test / Notes |
| LDL-C | Cholesterol in LDL particles | ASCVD event risk (moderate) | Widely used target; risk reduction with lowering documented. | Particle number varies; doesn’t measure plaque or inflammation. | Routine lipid panel; goals vary by risk (e.g. <100, 70, 55 mg/dL). |
| Non–HDL-C | Total cholesterol minus HDL-C (all apoB lipoprotein cholesterol) | ASCVD (often better than LDL-C) | Captures LDL+remnants+Lp(a) cholesterol; no extra test needed. | Can be raised by high TG; still a cholesterol measure. | Automatically from lipid panel; goal ≈30 mg/dL above LDL goal. |
| ApoB | Number of all atherogenic lipoprotein particles | ASCVD (stronger in metabolic risk) | Best single marker of particle burden; useful when LDL may be misleading. | Not measured in basic panel (costs more); few standard cutoffs. | If TG>200, diabetes, metabolic syndrome, CKD, or CVD: consider. |
| LDL-P | Number of LDL particles (via NMR) | ASCVD (similar to apoB) | Direct particle count; useful in statin-treated discordance. | Expensive; overlapping info with apoB; not routine. | Rarely – only if apoB not available and clinical scenario fits. |
| Lp(a) | A special LDL-like particle with apo(a) | Lifetime ASCVD risk (premature events) | Largely genetic and stable; independent risk factor. | Not lowered by statins/diet; measurement unit confusion (mg vs nmol). | Measure once in adulthood (or with strong family history); >50 mg/dL is high. |
| Triglycerides | TG in blood (reflects remnant lipoproteins) | ASCVD risk (if persistently high); pancreatitis risk if >500 mg/dL | Metabolic risk signal; routine test. | Highly variable; elevated by diet/illness; reflects broad metabolic state. | Every lipid panel. If >150–200 mg/dL, optimize weight/lifestyle. >500 mg/dL→treat to prevent pancreatitis. |
| hs-CRP | Systemic inflammation (C-reactive protein) | Residual ASCVD risk (modest) | Simple inflammation check; shows residual risk. | Very nonspecific; cannot “rule out” disease if low. | Optional in intermediate-risk patients or chronic inflammation. >2 mg/L is considered elevated. |
| Oxidized LDL | Oxidatively modified LDL | (Research) atherosclerotic activity | Reflects arterial oxidative stress. | Not standardized; no guidelines; expensive/experimental. | Not routine. Used only in research; ignore for everyday risk estimation. |
| CAC Score | Amount of calcified plaque in coronary arteries | Total atherosclerotic plaque/burden | Direct imaging of disease; powerful risk stratifier. | Cost, radiation; not for everyone; misses soft plaque. | If 40–75 yrs and risk borderline/intermediate, use CAC to guide statin decisions. CAC=0 implies very low near-term risk. |
Final Thoughts
If you have been told your LDL is too high, the most important takeaway is not that LDL means nothing. It is that LDL, on its own, does not tell you enough to understand what is really happening inside your arteries—important because the decision to start medication is not trivial.
Statins and other cholesterol-lowering drugs may have a place, but they are not something most people want to take lightly, especially when they can come with real downsides. Before making that kind of decision, it makes sense to ask whether a basic lipid panel has given you a full enough picture to justify it.
In many cases, it has not.
A high LDL result may be one clue that deserves attention, but it is still only one clue. It does not tell you about particle number, inherited risk, the wider metabolic environment, inflammatory burden, or whether plaque is already present. That is why markers like triglycerides, HDL, apoB, Lp(a), hs-CRP, and, in some cases, coronary artery calcium scoring can matter so much. They help move the conversation beyond a single number and closer to the real question: how concerned should you actually be?
That is the bigger point of this article. Not to tell you to ignore your doctor, and not to tell you what choice to make, but to help you see that one LDL result is rarely a complete enough basis for a confident decision on its own. If the stakes are high enough to involve lifelong medication, then the picture should be clear enough to justify it.
So the goal is not to fear LDL, and it is not to dismiss it. The goal is to put it back in its proper place: as one marker within a much larger story. Once you do that, your blood test becomes less of a verdict and more of a starting point. And that is a much better place from which to make an informed decision.
FAQs
What do LDL, HDL, and triglycerides actually measure?
LDL, HDL, and triglycerides each reflect a different part of fat transport and metabolism in the bloodstream. LDL carries cholesterol from the liver out to tissues that need it. HDL helps carry cholesterol back toward the liver for reuse or removal. Triglycerides are different: they are the main form of stored fat and often tell you more about energy balance and metabolic health than cholesterol transport alone. That is why these numbers appear together on the same lipid panel, but they are not all telling you the same story.
Is LDL cholesterol the most important number in a lipid panel?
LDL can be an important marker, but it is not enough on its own to give a full picture of cardiovascular risk. LDL-C tells you how much cholesterol is being carried inside LDL particles, but it does not tell you how many atherogenic particles are present, whether plaque is already forming, or what kind of inflammatory and metabolic environment those particles are moving through. That is why newer risk assessment often looks beyond LDL-C alone to markers like apoB, Lp(a), triglycerides, hs-CRP, and sometimes coronary artery calcium scoring.
Can you have normal LDL but still be at risk?
Yes. A “normal” LDL result does not automatically mean everything is fine. Someone can still carry meaningful cardiovascular risk if they have high triglycerides, low HDL, elevated apoB, raised Lp(a), persistent inflammation, insulin resistance, or evidence of plaque already developing in the arteries. In other words, LDL may look acceptable on paper while the wider risk picture is less reassuring. That is one reason a basic lipid panel can be useful without being definitive.