Only about 12% of American adults meet the criteria for optimal metabolic health. Even among adults at a “normal” body weight, fewer than one-third are metabolically healthy by that definition. In other words, metabolic dysfunction is not just a problem for people with obesity, diabetes, or obvious disease. It is often developing in people who look fine, feel mostly fine, and have been told their labs are “normal.”
That is what makes it so easy to miss.
Metabolic dysfunction rarely arrives as a sudden event. More often, it shows up as a slow drift: lower energy, stronger cravings, a growing waist, higher blood pressure, post-meal crashes, worse sleep, or fasting glucose sitting near the top of the normal range. None of this feels dramatic at first, so it gets blamed on age, stress, poor sleep, or being busy.
But metabolic health is not just about whether one number is technically normal. It is about how well your body handles energy — how it uses glucose, stores fat, responds to insulin, moves fats through the blood, protects the liver, regulates blood pressure, and keeps energy steady through the day.
This article explains the markers that actually matter, why they should be read together, and how to tell whether your metabolism looks resilient or whether your body is already compensating behind the scenes.
Metabolic Health Is How Well Your Body Handles Energy
The word metabolism comes from the Greek metabolē, meaning change, alteration, or transformation. And that really is the most useful way to think about it.
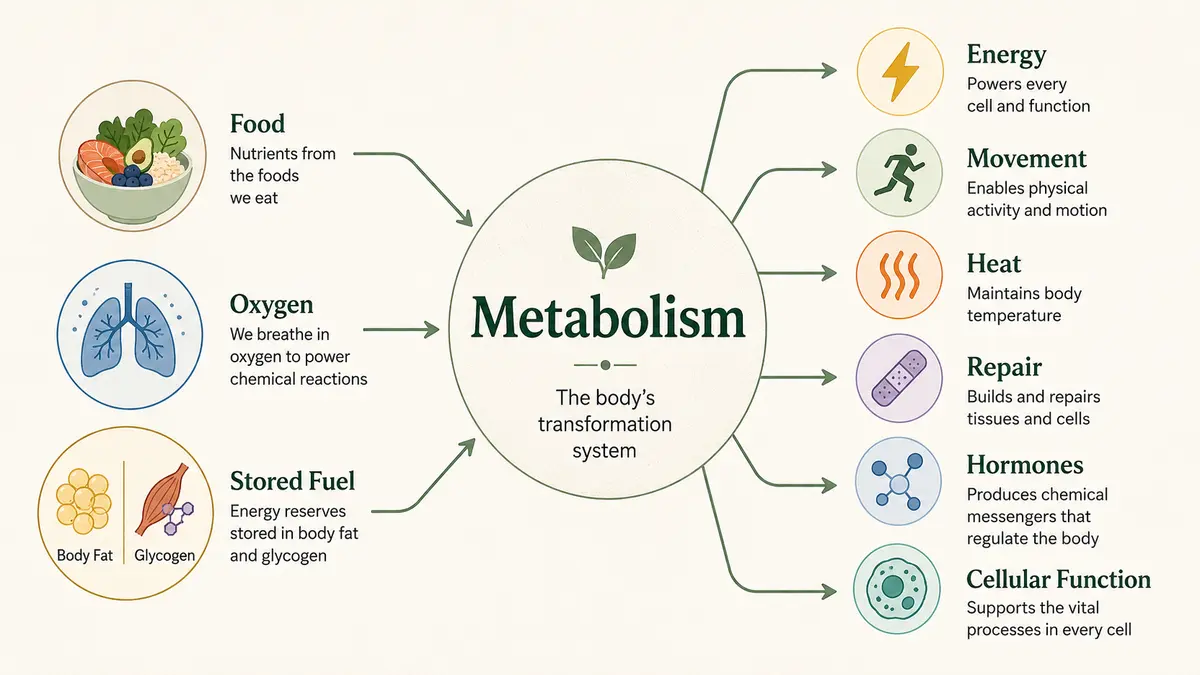
Contrary to most videos you seen on soical media, metabolism is not just how many calories you burn. It is the vast network of processes that transforms food, oxygen, stored fuel, and nutrients into energy, movement, heat, repair, hormones, and cellular function.
In other words, metabolism is the body’s conversion system — the machinery that allows life to keep adapting from one moment to the next. Ultimately, it’s about how well your body handles energy.
Your metabolism quietly manages energy in every situation your body has to deal with. It has to respond when you eat carbohydrates, protein, or fat. It has to adapt after a large meal, between meals, overnight, during exercise, during stress, and even during long periods without food. Whether you are walking around the house, lifting a heavy weight, running a marathon, recovering from illness, or simply sleeping, your body still needs energy. The ease with which your body can do this is known as metabolically flexibility.
A healthy metabolism can adjust to those different demands. It can use glucose when it’s available, burn fat when food is scarce, store energy safely after a meal, release energy when needed, and keep blood sugar reasonably stable through it all.
This is why metabolic health is not just about one lab number. A fasting glucose reading may still be “normal,” while the body is already producing more insulin than it should need to keep it there. The surface number can look fine, while the system underneath is working harder.
In simple terms, good metabolic health means your body can process, store, and use energy without needing constant compensation. Poor metabolic health begins when the body can still keep things looking normal, but only by working harder behind the scenes.
Metabolic Dysfunction Usually Starts Quietly
Metabolic dysfunction rarely begins with a dramatic diagnosis. More often, it starts as a slow drift: a little more fat around the waist, slightly higher blood pressure, triglycerides creeping up, lower energy after meals, stronger cravings, or fasting glucose sitting near the top of the “normal” range. Nothing looks urgent on its own, so it is easy to explain away as age, stress, poor sleep, or just being busy.
That quiet beginning is part of what makes metabolic dysfunction so easy to miss. The body is very good at keeping the surface numbers steady, even when the system underneath is under strain. And the modern health environment of desk jobs, poor sleep settings, and processed foods make this all the more subtle.
Blood sugar, for example, can remain in the normal range for years because the pancreas produces more insulin to keep it there. From the outside, the glucose reading may look reassuring. But internally, the body may already be working harder than it should to maintain that normal result.
The scale of the problem also shows how easily metabolic issues can hide in plain sight. One NHANES-based study found that only 12.2% of American adults met criteria for optimal metabolic health when waist circumference, glucose, blood pressure, triglycerides, HDL, and medication use were considered.
Even among normal-weight adults, fewer than one-third were metabolically healthy by that definition. The CDC also estimates that 115.2 million American adults have prediabetes, and about 8 in 10 do not know it.
And because the early effects are often familiar rather than frightening, many people adapt to them. Lower energy becomes “just getting older.” Afternoon crashes become normal. Constant snacking feels like a personality trait. A growing waist feels like an unavoidable part of adulthood. Cravings, poor sleep, and post-meal tiredness are blamed on stress or busyness.
Although none of these signs diagnose metabolic dysfunction by themselves, they appear regularly alongside changes in waist size, blood pressure, glucose, triglycerides, HDL, liver health, and other metabolic issues.
The point is not to panic over every number or symptom, but to notice the pattern early enough to do something about it. Metabolic health is easiest to protect before the body has spent years compensating.
Get Your Free Book!
Enter your email to get the free book and occasional updates from The New Health Order.
Normal Is Not Always Optimal
One of the easiest mistakes to make with metabolic health is assuming that “normal” means everything is working well. In medicine, normal ranges are often used to identify disease, classify risk, and decide when treatment may be needed. While useful, it is not the same thing as saying the body is functioning optimally.
A fasting glucose of 99 mg/dL is a useful example. Your doctor may tell you it is normal, and technically, they are correct: prediabetes begins at 100 mg/dL, while diabetes is diagnosed at 126 mg/dL or above. A1C is treated in a similar way, with anything below 5.7% considered normal. But the body does not suddenly become metabolically unhealthy the moment fasting glucose rises from 99 to 100 mg/dL. Metabolic dysfunction usually develops along a slope, not at a cliff edge.
That is where context changes the meaning. A fasting glucose of 99 mg/dL on its own does not prove metabolic dysfunction, but the same number alongside a growing waist, rising triglycerides, low HDL, higher blood pressure, fatty liver, cravings, or post-meal energy crashes deserves a closer look. That is not “normal”.
This is not just theoretical. In one large study of young men whose fasting glucose was still below the usual prediabetes cutoff of 100 mg/dL, those with fasting glucose of 91–99 mg/dL plus high triglycerides had about an eightfold higher risk of developing type 2 diabetes than men with lower glucose and lower triglycerides. A separate cohort found that people with fasting glucose of 95–99 mg/dL were more than twice as likely to develop diabetes as those below 85 mg/dL. So while a fasting glucose of 99 mg/dL may be technically normal, it can mean something very different when it appears alongside other signs of metabolic dysfunction.
This is especially important because metabolic dysfunction is often a pattern before it is a diagnosis. Blood sugar may still be normal because insulin is rising to keep it there. Triglycerides may still be close to range, but gradually moving upward. Blood pressure may not yet meet the definition of hypertension, but it may no longer be ideal. Waist size may creep up slowly enough that it feels like normal aging rather than a signal of changing energy storage.
That is why the standard metabolic syndrome markers are best read together. Metabolic syndrome is usually diagnosed when someone has three or more of the following: a large waist circumference, high blood pressure, high fasting glucose, high triglycerides, or low HDL cholesterol. But those markers do not suddenly become meaningful only once three boxes are checked. Even one or two moving in the wrong direction can be an early clue that the body is starting to work harder to maintain stability.
This does not mean every high-normal number is a crisis. It means the trend and the context matter. A single fasting glucose reading of 99 mg/dL after poor sleep, stress, illness, or a late meal is not the same as consistently high-normal glucose alongside a growing waist, rising triglycerides, low HDL, higher blood pressure, and low energy after meals.
The Main Markers of Metabolic Health
Because one measure can underplay the level of metabolic dysfunction across the whole body, your total metabolic health profile is best understood as a pattern, not a single number. The classic medical framework is metabolic syndrome, which looks at five main markers: waist circumference, blood pressure, fasting glucose, triglycerides, and HDL cholesterol.
The American Heart Association describes metabolic syndrome as being diagnosed when someone has three or more of these risk factors. But even before someone meets the formal definition, these markers can still reveal whether the body is beginning to struggle with energy handling.
Waist Size
One of the best tests is actually one of the simplest – waist size. Waist size matters because where fat is stored often tells us more than body weight alone. Fat stored around the abdomen is more closely linked with insulin resistance, fatty liver, higher triglycerides, high blood pressure, type 2 diabetes, and cardiovascular risk than fat stored more evenly under the skin.
This is why someone can have a “normal” body weight but still be metabolically unhealthy, while another person with a higher body weight may have better markers than expected. BMI can be useful at a population level, but it does not tell you where fat is stored, how much muscle someone has, or whether their blood pressure, glucose, triglycerides, HDL, and liver markers are healthy.
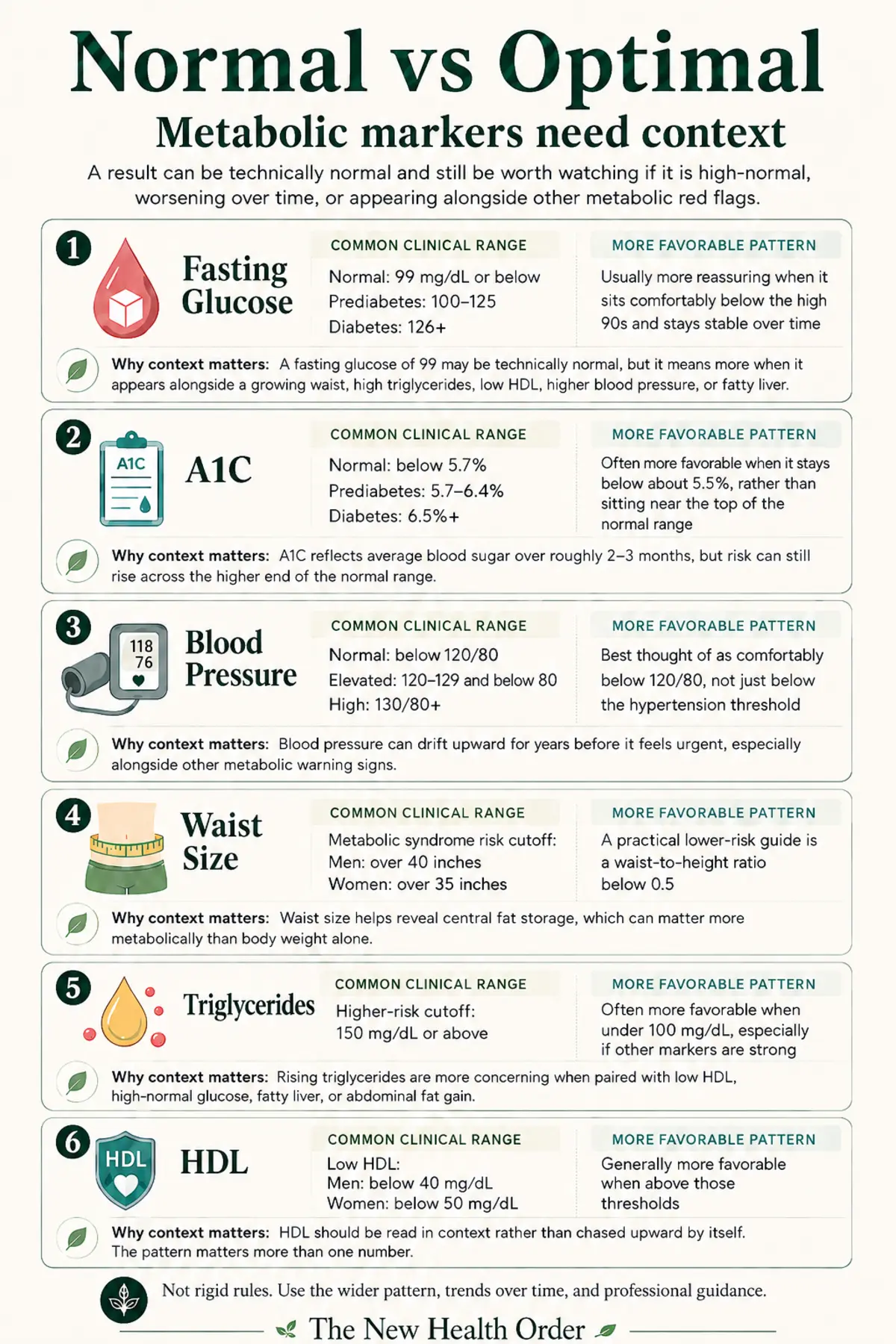
For metabolic syndrome, the American Heart Association uses waist circumference cutoffs of greater than 40 inches for men and greater than 35 inches for women as one of the diagnostic risk factors. These are not perfect individual targets, but they show why central fat gain deserves attention.
Blood Pressure
Blood pressure is often treated as a heart-health marker, but it also belongs in the metabolic picture. High blood pressure is one of the core features of metabolic syndrome, and it often appears alongside insulin resistance, abdominal fat gain, poor sleep, stress, kidney strain, and worsening blood sugar regulation.
The important point is that blood pressure does not need to be severely high before it matters. Under the ACC/AHA categories, normal blood pressure is below 120/80 mm Hg, elevated blood pressure is 120–129 systolic and below 80 diastolic, stage 1 hypertension begins at 130–139 systolic or 80–89 diastolic, and stage 2 hypertension begins at 140/90 mm Hg or above.
So if someone’s blood pressure has slowly moved from 110/70 to 128/82, that may not feel dramatic, but it is still a meaningful change. As with every metabolic marker, the context matters. A borderline number in isolation is one thing; a borderline number alongside a growing waist, high triglycerides, poor sleep, and rising glucose tells a different story.
Fasting Glucose and A1C
Fasting glucose and A1C are two of the most common ways doctors assess blood sugar control. Fasting glucose shows what blood sugar looks like after an overnight fast. A1C gives a rough picture of average blood sugar over the past two to three months. The CDC classifies fasting glucose of 99 mg/dL or below as normal, 100–125 mg/dL as prediabetes, and 126 mg/dL or above as diabetes. For A1C, below 5.7% is normal, 5.7–6.4% is prediabetes, and 6.5% or above is diabetes.
These numbers are useful, but they are incomplete. Fasting glucose can look normal even when the body is using more insulin than it should need to keep it there. A1C can also miss daily spikes and dips because it reflects an average. The CDC itself notes that A1C does not replace understanding how blood sugar changes throughout the day, and that several factors can affect A1C accuracy, including anemia, kidney failure, liver disease, certain blood disorders, pregnancy, blood loss, and some medicines.
So the question is not only, “Is my glucose normal?” It is also, “Is my glucose stable, is it trending upward, and what other markers are changing with it?”
Triglycerides and HDL
Triglycerides and HDL are often placed inside the cholesterol panel, but they are also metabolic markers. Triglycerides are a form of fat carried in the blood. They often rise when the body is struggling with excess energy, insulin resistance, refined carbohydrate intake, alcohol intake, or fatty liver. HDL is more complicated than the simple phrase “good cholesterol,” but low HDL often appears as part of the same metabolic pattern as high triglycerides, abdominal fat, and insulin resistance.
For metabolic syndrome, the American Heart Association uses triglycerides of 150 mg/dL or higher and low HDL cholesterol — below 40 mg/dL for men or below 50 mg/dL for women — as two of the diagnostic risk factors. That does not mean 149 mg/dL is automatically ideal. In the Framingham Offspring Study, cardiovascular risk was higher when low HDL appeared alongside triglycerides of 100 mg/dL or higher, which is why triglycerides below 100 mg/dL are often viewed as a more favorable metabolic pattern, even though 150 mg/dL remains the formal clinical cutoff.
The pattern matters more than either number alone. High triglycerides with low HDL can suggest that the body is not handling energy and fat transport well. It does not prove one specific cause, and it should not be interpreted in isolation, but it can be a useful warning sign when it appears alongside waist gain, high-normal glucose, high blood pressure, or suspected fatty liver.
Insulin Resistance
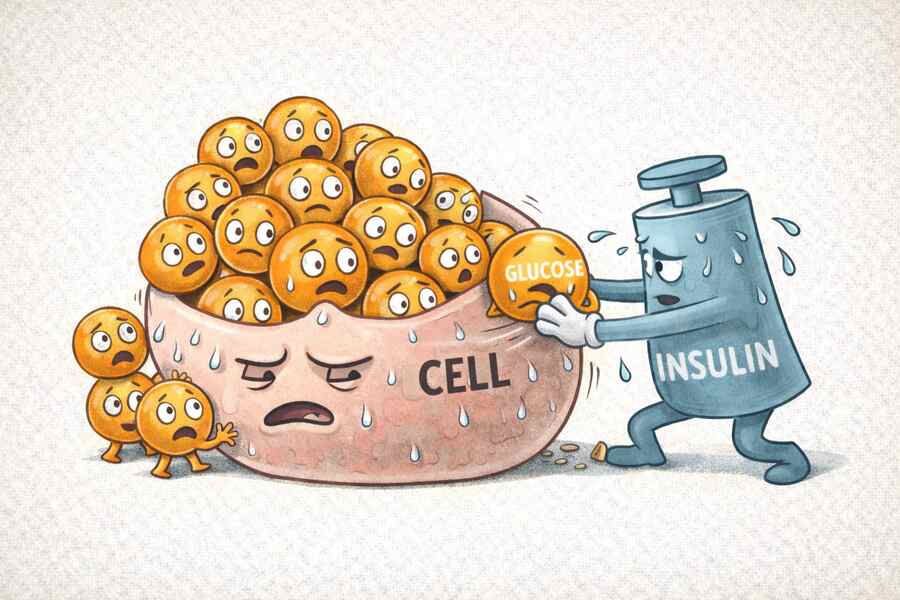
Insulin resistance is one of the most important ideas in metabolic health because it helps explain how dysfunction can begin before glucose looks clearly abnormal. Insulin is the hormone that helps move glucose out of the bloodstream and into cells. Insulin resistance means the body’s muscle, fat, and liver cells do not respond to insulin as well as they should, so the body has to produce more insulin to get the same effect.
This is why normal fasting glucose can sometimes be misleading. The glucose number may still look acceptable because insulin is doing extra work behind the scenes. Over time, if the body cannot keep compensating, blood sugar may begin to rise into prediabetes or diabetes.
One problem is that insulin resistance is not always measured directly in routine care. The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) notes that health care professionals may not test for insulin resistance, and that insulin resistance testing is primarily used in research settings. Instead, doctors usually rely on blood glucose tests, A1C, lipid markers, blood pressure, waist size, and clinical context.
That does not make insulin resistance unimportant. It means many people have to infer it from the broader pattern unless their doctor specifically orders fasting insulin, HOMA-IR, an oral glucose tolerance test, or other more detailed testing.
For a deeper look at insulin resistance and its role in metabolic health, see this article here.
Fatty Liver
Fatty liver is one of the most important metabolic warning signs because it shows that excess energy is being stored in an organ that is not meant to become a long-term fat depot. NIDDK defines Nonalcoholic Fatty Liver Disease (NAFLD), now also referred to as MASLD, as a condition where excess fat builds up in the liver when that fat buildup is not caused by heavy alcohol use.
Fatty liver is often quiet. NAFLD usually has few or no symptoms, which makes it easy to miss unless liver enzymes, imaging, or other clinical clues bring it to attention. It is also closely connected to the rest of the metabolic picture: overweight or obesity, insulin resistance, type 2 diabetes, high triglycerides, abnormal cholesterol, and metabolic syndrome all increase the likelihood of fatty liver.
This is why fatty liver should not be seen as only a liver problem. In many cases, it is a sign that the body’s energy-storage system is under strain. The liver is receiving, making, or storing more fat than it can comfortably handle.
Energy, Hunger, and Cravings
Not every metabolic marker comes from a blood test. How someone feels through the day can also provide useful context, even though symptoms are not diagnostic by themselves.
Energy crashes after meals, frequent hunger, strong cravings, difficulty going several hours without food, post-meal sleepiness, and reduced exercise tolerance can all have many causes. Poor sleep, stress, thyroid issues, anemia, under-eating, overtraining, medications, and other health problems can produce similar symptoms. So these signs should not be used to self-diagnose metabolic dysfunction.
But they should not be ignored either. People with insulin resistance and prediabetes usually have no symptoms, which is exactly why metabolic dysfunction can develop quietly. When subjective symptoms do appear alongside objective changes — a growing waist, rising blood pressure, high-normal glucose, high triglycerides, low HDL, or fatty liver — they become part of the bigger pattern.
The point is not to panic over tiredness or cravings. The point is to stop dismissing every change as just getting older. If your numbers are drifting and your daily energy is getting worse, your metabolism may be asking for attention before a formal diagnosis arrives.
The Pattern Matters More Than One Number
By now I hope you have taken away that metabolic health is not judged well from a single marker in isolation. One blood test, one waist measurement, or one slightly abnormal result can be useful, but it rarely tells the whole story. The real value comes from looking at how the markers fit together.
A fasting glucose of 99 mg/dL may still fall inside the normal range. On its own, that does not prove metabolic dysfunction. But if that same person also has rising triglycerides, falling HDL, a growing waist, higher blood pressure, and low energy after meals, the meaning changes. The glucose number is no longer just a single result. It becomes part of a pattern.
Metabolic Patterns Worth Paying Attention To
| Pattern | What it may suggest |
| High-normal fasting glucose + high triglycerides + growing waist | Possible early insulin resistance or poor energy handling |
| Normal glucose + high triglycerides + low HDL | Blood sugar may look fine, while lipid metabolism is already strained |
| Normal BMI + large waist | Body weight may be hiding central fat storage |
| Fatty liver + high triglycerides | Possible energy overflow into the liver |
| Energy crashes + cravings + rising waist | Not diagnostic, but worth reading alongside objective markers |
| One abnormal marker but everything else strong | Context matters; one number should not be overinterpreted |
That is why metabolic syndrome is built around a cluster of markers rather than one measurement. Waist size, blood pressure, fasting glucose, triglycerides, and HDL are different signals, but they often move together because they are connected to the same underlying problem: the body is struggling to handle, store, and regulate energy efficiently.
This also works in the other direction. A person may have one marker outside the ideal range, but if everything else looks strong ((keto and carnivore dieters often have a high LDL level while every other marker looks good) — waist size, blood pressure, glucose, triglycerides, HDL, liver markers, energy, appetite, and fitness — the interpretation may be different. Context does not make the marker irrelevant, but it helps prevent overreacting to one number.
Trends matter too. A marker that is technically normal but steadily worsening over several years may deserve more attention than a slightly abnormal result that is stable, explainable, or improving. A waist measurement slowly increasing, blood pressure gradually rising, triglycerides creeping upward, or fasting glucose moving from the low 80s to the high 90s can all be early signs that the body is drifting toward dysfunction.
How to Pull the Markers Together
The point of understanding these markers is not to turn metabolic health into a source of anxiety. It is to stop looking at each number in isolation and start seeing the wider pattern.
A good place to begin is with the basic markers: waist size, blood pressure, fasting glucose, A1C, triglycerides, and HDL cholesterol. These are not perfect, but together they give a useful first picture of how well your body is handling energy. If several of them are drifting in the wrong direction, that matters more than one borderline number on its own.
The next step is to compare “normal” with “optimal.” A result can sit inside the official reference range and still be worth watching if it is consistently high-normal, worsening over time, or appearing alongside other warning signs. Fasting glucose near the top of the normal range means something different when it comes with high triglycerides, low HDL, rising blood pressure, a growing waist, or symptoms such as post-meal crashes and frequent cravings.
This is where context matters. One poor night of sleep, a stressful week, illness, alcohol, a late meal, or a hard workout can all affect certain markers. You do not need to panic over one reading. What you want to know is whether your overall pattern is stable, improving, or slowly moving toward dysfunction.
If you want a clearer picture, it may be worth discussing additional markers with your doctor, especially fasting insulin, HOMA-IR, liver enzymes, or further testing if fatty liver is suspected. These are not always part of routine bloodwork, but they can add useful context when the basic markers do not explain what you are seeing or feeling.
The same applies to daily symptoms. Energy crashes, constant hunger, intense cravings, poor sleep, and needing caffeine to feel normal do not diagnose metabolic dysfunction. But if they appear alongside changes in waist size, glucose, blood pressure, triglycerides, HDL, or liver markers, they become part of the story.
The aim is not to chase perfect numbers. It is to understand your baseline, watch the trend, and act early enough that small changes do not become permanent diagnoses. Better metabolic health usually shows up as a quieter, more resilient system: steadier energy, better appetite control, improved waist size, healthier blood pressure, better glucose regulation, lower triglycerides, improved HDL patterns, and less need for the body to compensate in the background.
That is the practical takeaway: do not ask only whether your labs are “normal.” Ask whether your metabolism looks resilient, whether the pattern is moving in the right direction, and whether your body is handling energy with ease or strain.
FAQs
What is metabolic health?
Metabolic health describes how well your body handles energy. It includes how your body uses glucose, stores fat, responds to insulin, moves fats through the blood, regulates blood pressure, protects the liver, and keeps energy stable through the day. Good metabolic health means these systems work without the body needing constant compensation.
What are the main markers of metabolic health?
The main markers include waist size, blood pressure, fasting glucose, A1C, triglycerides, HDL cholesterol, insulin resistance, fatty liver, and daily patterns such as energy, hunger, and cravings. No single marker tells the whole story. The most useful picture comes from reading them together.
Can your labs be normal but your metabolic health still be poor?
Yes. A lab result can be technically normal and still be worth watching if it is high-normal, worsening over time, or appearing alongside other warning signs. For example, fasting glucose may still fall inside the normal range while insulin, triglycerides, waist size, blood pressure, or fatty liver risk are already moving in the wrong direction.